

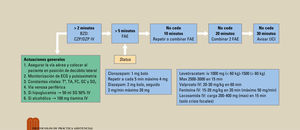
Las crisis epilépticas representan entre el 1%-2% de las consultas al servicio de urgencias. No toda crisis es epilepsia. Hay 4 tipos de escenarios. Por un lado, está la crisis aguda sintomática secundaria a un proceso orgánico o a daño agudo en el sistema nervioso central (SNC). Deberemos identificar la causa e iniciar tratamiento hasta la resolución de la misma. En segundo lugar, está la primera crisis no provocada. Se debe hacer anamnesis, exploración y pruebas complementarias, incluyendo tomografía computarizada (TC) cerebral y electroencefalograma (EEG). No se debe iniciar tratamiento salvo que haya alteraciones en neuroimagen o en el EEG o se presente crisis nocturna o daño preexistente en el SNC, dado que aumenta el riesgo de recurrencia. En tercer lugar, está el paciente epiléptico conocido, en el que debe realizarse una anamnesis de control previo a la crisis y posibles desencadenantes. No precisa TC ni EEG, salvo cambio en el formato de las crisis. Hay que valorar tratar el factor desencadenante y el ajuste de dosis de los anticomiciales. Por último, podemos encontrar el estado epiléptico. Se trata de crisis recurrentes o no recuperación completa del nivel de conciencia entre las crisis. Se debe estudiar la causa y tratar precozmente con benzodiacepinas, asociando tratamiento antiepiléptico a los 5 minutos del inicio y valoración por cuidados intensivos si no se produce una mejoría a los 20 minutos del inicio.
Palabras clave
Epileptic seizures account for 1%-2% of emergency department consultations. Not every seizure is epilepsy. There are four types of scenarios. The first is an acute symptomatic crisis secondary to an organic disease or acute central nervous system injury. The cause must be identified and treatment initiated until it resolves. The second is first unprovoked seizure. A case history, examination, and additional tests must be performed, including a brain computed tomography (CT) scan and electroencephalogram (EEG). Treatment should not be started unless there are neuroimaging or EEG abnormalities or if there are nocturnal seizures or pre-existing central nervous system (CNS) injury, as these aspects increase the risk of recurrence. The third type is the known epileptic patient. For these individuals, a follow-up case history should be performed prior to the seizure and possible triggers. These patients do not require a CT scan or an EEG unless there is a change in the nature of the seizures. Treating the triggering factor and adjusting the dose of anticonvulsants should be considered. Lastly, there is status epilepticus. These are recurrent seizures or a lack of full recovery of level of consciousness between seizures. The cause must be studied and treated early with benzodiazepines, associating antiepileptic treatment within five minutes of onset. The patient should be evaluated by the intensive care department if there is no improvement within 20minutes of onset.
Keywords
Identifíquese
¿Aún no es suscriptor de la revista?

Comprar el acceso al artículo
Comprando el artículo el pdf del mismo podrá ser descargado
Teléfono para incidencias
De lunes a viernes de 9h a 18h (GMT+1) excepto los meses de julio y agosto que será de 9 a 15h